Gastric sleeve Perth
Gareth had gastric sleeve surgery and now lives an active life

Gastric
sleeve
Expected excess weight loss:
60 - 70 %Average procedure time:
45 - 60 minutesAverage recovery time:
2 weeksGastric sleeve
Laparoscopic Sleeve Gastrectomy is the most common bariatric operation performed in Australia to achieve weight loss. Invented by accident in 1998 by Michel Gangner in the United States, this weight loss surgery has been constantly refined over the past twenty years.
In the right hands, a well-constructed sleeve gastrectomy is a powerful and safe weight loss tool.
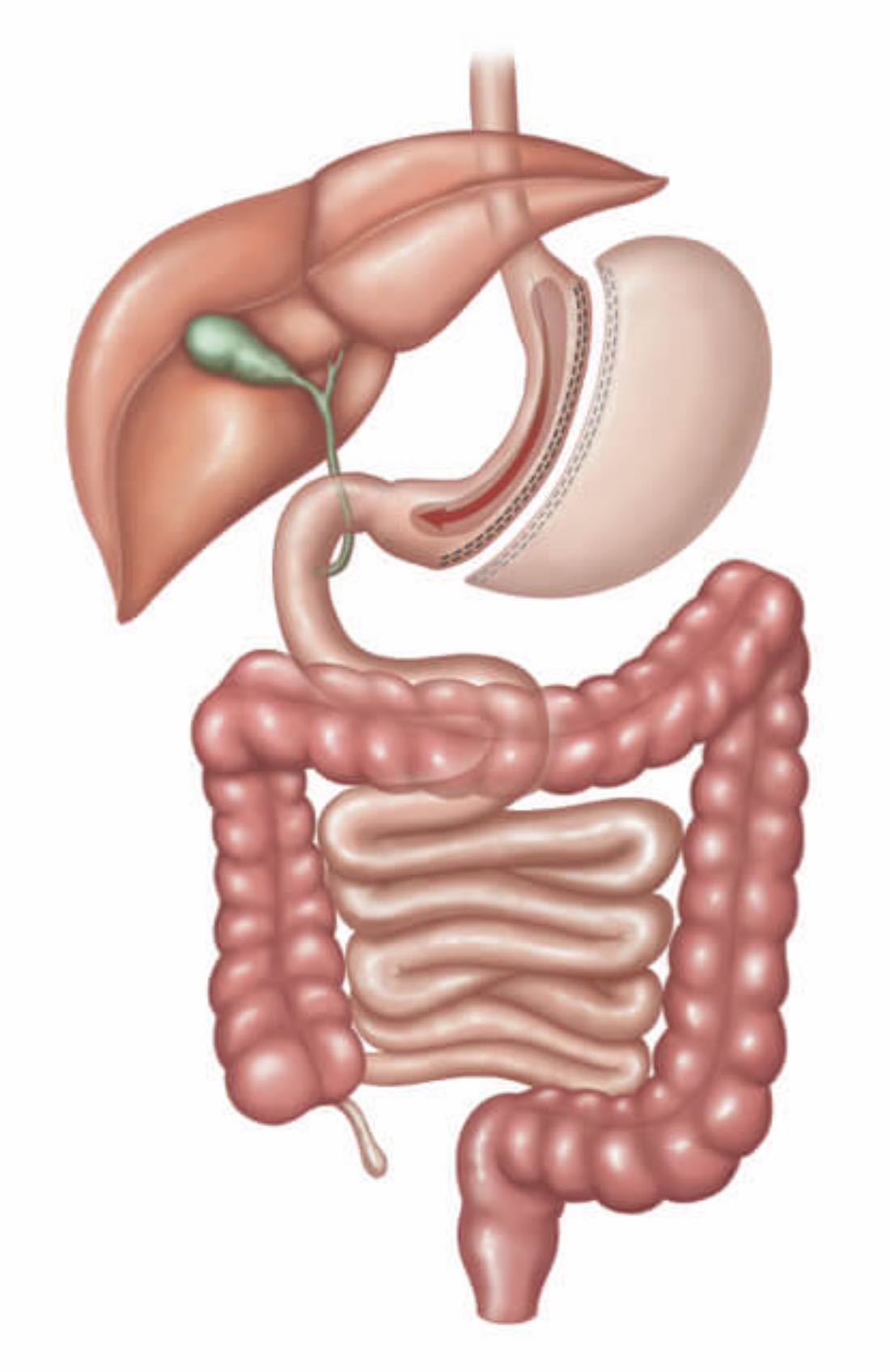
What is a gastric sleeve?
A sleeve gastrectomy is a surgical procedure that reduces the size of the stomach to about 150mls. The outer margin of the stomach is removed after a ‘sleeve’ of stomach is created, using a surgical stapler and a tubular sizing device known as a “bougie”.
The exact volume is hard to measure as the stomach is very elastic and can easily stretch. However, an experienced bariatric surgeon is able to understand this and compensate.
Getting the size of the stomach sleeve correct is important. If the stomach volume is too large, you won’t lose enough weight. Too small, and you develop the risk of gastric sleeve complications such as a stricture or kink, which causes terrible vomiting.
Other factors to take into account are previous surgeries, the amount of inherent stomach spasm, and how much weight loss is actually required.

Benefits of a gastric sleeve?
The best thing about a sleeve gastrectomy is that it’s a straightforward surgery to perform, with many additional benefits. It restricts only the amount of food you can consume, and NOT the types of foods you can eat - as is the case with the gastric band procedure. It also does NOT cause any malabsorption, and the expected weight loss results are comparable to a RNY Gastric Bypass.
Video: Perth bariatric surgeon Dr Harsha Chandraratna explains the benefits of a sleeve gastrectomy
What techniques are available to perform gastric sleeve surgery
In our Perth practice we aim to perform sleeve gastrectomy using laparoscopic (keyhole) surgery. We find this technique very effective. A major advantage is that our clients recover quickly.
Very occasionally, we will need to revert to open surgery with a large incision on the abdomen (a laparotomy). For some people, this may be the only way to proceed with the procedure.
If you have had previous major abdominal surgery, especially in the upper abdomen, open surgery may be an option your surgeon will discuss with you. In the past ten years of our practice, we have only had to do this twice. More often than not, we succeed with keyhole surgery.
Robotic surgery is an exciting upcoming option. I suspect it won’t be helpful for patients seeking a sleeve gastrectomy, but for more complex procedures like gastric bypasses it may play an important role. The current problem is that the cost of the disposable equipment for the robot would add an extra $2500 to each case. However, this price may decrease in the near future as the surgery becomes more common.
How do we perform the surgery?
Once you are asleep under anaesthesia, we will place antiseptic on your abdomen and cover you in sterile surgical drapes (just like you have seen on TV).
Your surgeon will make a small incision in the skin and very carefully insert a small tube through your stomach wall and into your abdomen. Once through the abdominal wall layer, the surgeon will inflate your abdomen with carbon dioxide gas, place a camera through the tube in your stomach, and perform an initial visual assessment.
Once the surgeon is happy that everything is as it should be, they will place three other tubes into your abdomen. These are to pass the instruments through to perform the surgery. A fifth hole, just under the ribs, will be made so that the Nathanson liver retractor can be placed in the abdominal cavity. This will hold the liver out of the way.
Importance of Optifast
This is where the pre-operative Optifast diet is very important. Patients who haven't done the diet will have a lot of fat in their liver. This makes the liver very hard to lift.
In this situation, the liver can also be very brittle and it is possible to tear or damage it. This can lead to serious complications during and after the surgery.
Once the ports are in and the liver is lifted out of the way, we are ready to begin the surgery.
The first step is to free the stomach of all its attachments. Using an electrosurgical device, the surgeon will cut and seal all the vessels feeding the stomach along the greater curve (the left-hand side of the stomach). We start from the very bottom, near the pylorus, and continue right up to the top, near the oesophagus. At the top, the small vessels connecting the stomach to the spleen will be divided.
Once the stomach is free, the anaesthetist will pass a bougie (a calibration tube) through your mouth, down the oesophagus, and into the stomach. With the surgeon’s help, your anaesthetist will then pass the bougie through the pylorus at the bottom of your stomach and out into the duodenum.
The surgical assistant will then pull the stomach to the left and carefully make sure there is no stomach hiding that may escape the stapler and leave a pouch. Next, the surgeon manipulates the stapler into the correct position and uses it to divide and seal the stomach. It takes, on average, six firings of the stapling device to complete the sleeve.
What are the staples made of?
What is the MiniMizer gastric ring?
Cost MiniMizer Ring

Does medicare cover gastric sleeve in Australia?
There is some rebate from Medicare for the gastric sleeve. They will pay approximately $675 for a sleeve gastrectomy. This amount is usually paid directly to your surgeon.
Medicare will not pay for your hospital stay or any consumables used. They will pay some money towards your medications and any tests you may require.
As you can see, it’s a little complicated. Our clinic staff can provide more information to simplify things for you as much as possible. If they don’t have all the necessary answers, they will direct you to the people who can answer your questions accurately.
Is a sleeve gastrectomy procedure covered by your private health insurance?
Sleeve gastrectomy (and all of our surgical procedures) are covered by private health insurance. However, you will have to check that it is covered by your particular level of health insurance cover. In the latest Federal Government overhaul of the Australian private health insurance industry bariatric surgery has been moved to the gold level of cover only.
It is important to know that different health funds do have different rules. So it is critical that you ring your private health fund and quote the appropriate number for the procedure you prefer, to confirm that it will be covered by your insurance policy.
Video: What can I eat after Sleeve Gastrectomy surgery?
About Obesity Surgery WA: Our 6 commitments
Taking surgery seriously
We know that entering into an operation is a big deal and we are very serious in getting the best outcome for you. We practice what is considered to be a world class standard. Our staff regularly attend national and international conferences and bring back what is the latest research and technology.Running on time
Our Surgeons and all of our staff try their best to run on time. Although it's not always possible, our commitment is that we do our best. Your time is valuable and we respect that.Readily available
Our surgeons (or at least one of them) are always available in a crisis. Some of them may provide you with a direct contact, but all are available through the hospital switchboard and happy to chat any time if there is a crisis.An obsessive attention to detail
We do our best to not miss anything. Every stitch, every staple and every clip is applied to exactly where it needs to be with the greatest care possible.Commitment to performing the best operation possible
Not all operations are the same and there a few extras that we do to make things better. We know that our results are better with the minimiser ring so we offer it to everyone. We know that reflux can be an issue so we try to tighten every oesophageal hiatus to make reflux control as good as possibly can be.Useful links
Weight loss
surgery
Obesity
Bariatric
diet
Meet our team

Dr. Harsha Chandraratna
Consultant Surgeon
MBBS FRACS